Rotator cuff injuries are extremely common and can be the result of acute traumatic injuries or degenerative age-related changes. They can be very debilitating, greatly affecting sleep and daily activity such as washing your hair or making a cup of tea, as well as limiting sporting activity. Prompt diagnosis is paramount to guide effective treatment and help ensure a quick recovery.
London Sports Physiotherapy is very unique in that we offer diagnostic ultrasound scans within consultations. This helps us to visualise your rotator cuff and provide an instant definitive diagnosis that informs and guides your treatment.
This blog provides an in-depth look at the factors that matter most with rotator cuff injuries and rotator cuff tears.
If you think you have experienced a rotator cuff shoulder injury or if you would like an assessment from one of our expert physiotherapist’s to rule out a tear, do not hesitate to book your appointment today.
1. What Is Rotator Cuff Related Shoulder Pain?
The shoulder is the most mobile joint in the human body, capable of movement across a greater range than any other joint. As a result of this vast mobility, stability is highly compromised meaning shoulders are highly prone to injuries such as a rotator cuff tears, impingement, subluxation or in extreme cases, dislocation. The rotator cuff muscle group provide dynamic muscular control and primary stabilisation that keeps the shoulder both functional and protected.
Rotator cuff related shoulder pain (RCRSP) is an umbrella term that encompasses a spectrum of conditions affecting the rotator cuff tendons and the surrounding structures, including rotator cuff tendinopathy, subacromial pain syndrome, and partial or full-thickness rotator cuff tears. It is one of the most prevalent musculoskeletal complaints seen in clinical practice and a leading cause of shoulder pain in adults across Sutton, South London and the UK.
Understanding the anatomy of the shoulder and the specific role of the rotator cuff is essential to appreciating why these injuries occur, how they present, and critically why the vast majority respond extremely well to expert physiotherapy without the need for surgery.
The Anatomy of the Shoulder
The shoulder complex is made up of three bones, the humerus (upper arm bone), the scapula (shoulder blade), and the clavicle (collarbone), and three articulating joints: the glenohumeral joint, the acromioclavicular joint, and the sternoclavicular joint. The glenohumeral joint is the primary “ball and socket” joint of the shoulder, where the rounded head of the humerus articulates with the shallow glenoid fossa of the scapula. Because the glenoid is relatively flat (often compared to a golf ball resting on a tee) the joint relies heavily on the surrounding soft tissues for stability.
The Rotator Cuff as a Stabiliser
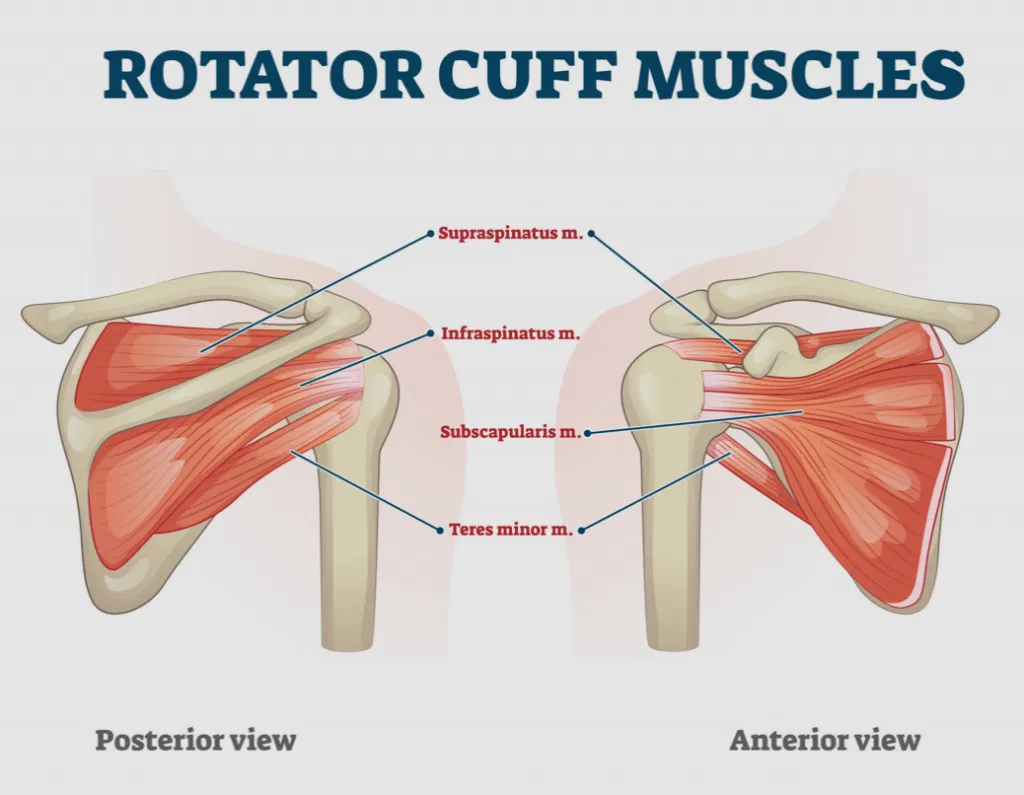
The rotator cuff consists of four muscles and their tendons, the supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles originate from the scapula and insert around the humeral head, forming a cuff of tissue that encases the joint. Working in tandem, they produce specific shoulder movements and act as dynamic stabilisers of the glenohumeral joint by compressing the humeral head into the glenoid throughout movement, a mechanism known as the force couple.
The supraspinatus muscle initiates and assists shoulder abduction. Infraspinatus and teres minor are the primary external rotators of the shoulder. Subscapularis, the largest of the four, is the principal internal rotator and also plays a crucial role in anterior shoulder stability.
Whilst the four rotator cuff muscles have differing roles during shoulder movement, they never work in isolation, always together as a team, just not always in equal parts.
When the rotator cuff is healthy and functioning optimally, the humeral head remains centred in the glenoid during all movement. When it is compromised (via injury, degeneration, pain inhibition, or muscle imbalance) this centring mechanism is disrupted, leading to abnormal joint mechanics, tissue overload, and often pain.
2. What Causes Rotator Cuff Injuries?
Rotator cuff injuries occur across a wide age range and arise through two broad mechanisms: acute traumatic injury and gradual degenerative change.
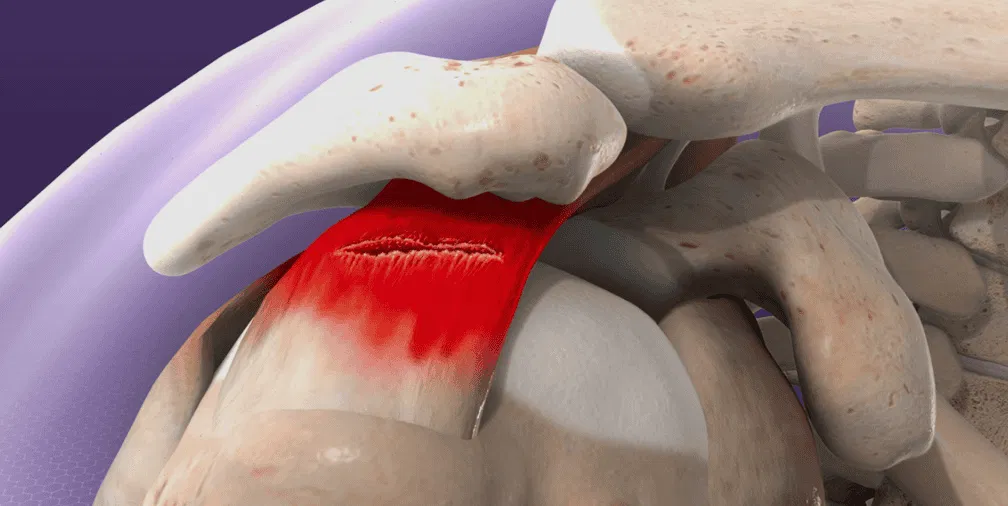
Acute tears typically occur following a sudden forceful event such as a fall onto an outstretched arm, a heavy lifting incident, or a contact sports collision, and are more common in younger, active individuals. The supraspinatus tendon is the most commonly involved in acute injury due to its anatomical position and the compressive forces it experiences beneath the coracoacromial arch.
Degenerative tears develop gradually over time and are strongly associated with increasing age, repetitive overhead activity, and cumulative mechanical loading. Tendon blood supply diminishes with age, particularly in the critical zone of the supraspinatus, a region of relative avascularity approximately 1 cm from the tendon insertion, making this area particularly vulnerable to degenerative change. Degenerative tears are frequently seen in the fifth decade and beyond, and are often asymptomatic initially.
Other contributing factors may include rotator cuff muscle imbalance, poor scapular control (scapular dyskinesis), acromial morphology (a hooked or curved acromion reduces the subacromial space and increases impingement), repetitive overhead sport or occupation, and a history of shoulder trauma or prior episodes of shoulder pain. We say “may” as it is not uncommon for these findings to be identified and present without pain or symptoms, rendering them incidental and not related to the clients presenting pain. This is why an assessment by a skilled and experienced physiotherapist is vital in identifying your primary pain driver.
3. Signs and Symptoms of Rotator Cuff Related Shoulder Pain
The symptoms of rotator cuff related shoulder pain vary according to the specific structure involved, the severity of the pathology, and whether the presentation is acute or chronic.
Common presentations include a dull, aching pain in the outer aspect of the shoulder and upper arm, which is typically worse with overhead activities, reaching behind the back, or lying on the affected side at night. Night pain is a particularly characteristic feature and frequently disrupts sleep, a significant impact on quality of life.
A painful arc of movement (pain occurring between approximately 60 and 120 degrees of shoulder abduction) is a classical clinical finding associated with subacromial impingement and supraspinatus tendinopathy. Weakness with specific movements such as external rotation or resisted abduction may suggest a significant tear. A sensation of clicking, catching, or clunking may indicate structural pathology within the joint. Special Orthopaedic tests (which are not so special but that’s a blog for a different day) such as the Hawkins-Kennedy test or Open and Empty Can tests may be positive.
In cases of large or complete tears, there may be visible muscle wasting in the supraspinatus or infraspinatus fossa, and marked functional limitation with an inability to lift the arm without compensatory shrugging.
4. How Are Rotator Cuff Injuries Diagnosed?
Accurate diagnosis requires a detailed clinical assessment and, in many cases, the addition of targeted imaging such as point-of-care diagnostic ultrasound scans offered here at London Sports Phystiotherapy in Sutton, to confirm the nature and extent of any structural pathology.
Our expert clinicians conduct a thorough subjective history, exploring the mechanism of onset, behaviour of symptoms, aggravating and easing factors, and functional limitations. This is followed by a comprehensive physical examination, including assessment of active and passive range of motion, specific orthopaedic tests ( Hawkins-Kennedy test, Neer’s sign, the empty can test, Gerber’s lift-off test, and the external rotation lag sign) and careful palpation of the relevant structures.
Objective strength testing using our state-of-the-art VALD dynamometry equipment can provide precise, quantifiable data on rotator cuff and surrounding muscle strength, enabling us to identify specific deficits, measure side-to-side asymmetries, and establish a clear baseline for monitoring rehabilitation progress. This level of detail elevates the quality of assessment and ensures that treatment is targeted, evidence-based, and measurable from the very first session.
Where imaging is indicated, diagnostic ultrasound offers a dynamic, real-time assessment of tendon structure and is highly effective for identifying partial and full-thickness tears.
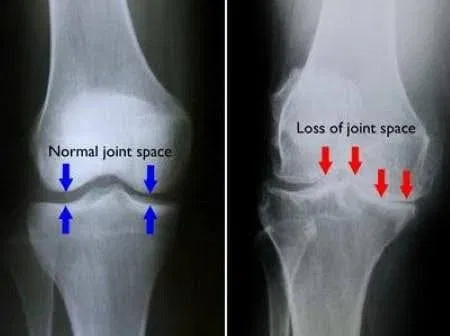
MRI provides the gold standard for soft tissue assessment, clearly delineating tendon integrity, tear size, location, and the degree of any associated muscle atrophy or fatty infiltration. X-ray may also be used to assess bony anatomy, including acromial morphology and the degree of any glenohumeral or acromioclavicular joint degeneration (osteoarthritis).
Tear Location and Its Impact on Treatment
The location and characteristics of a rotator cuff tear have a direct bearing on treatment planning, and our clinicians take these factors into careful consideration.
Partial-thickness tears may occur on the bursal surface (the upper aspect of the tendon, facing the subacromial bursa) or on the articular surface (the lower aspect, facing the glenohumeral joint). Articular-sided partial tears are the more common of the two and are frequently associated with overhead sport and repetitive activity. Both types of partial tears carry an excellent prognosis with conservative management in the majority of cases.
Full-thickness tears represent a complete disruption of the tendon from its bursal to articular surface. They range from small (less than 1 cm) to massive (involving two or more tendons). Small and medium full-thickness tears, particularly in the supraspinatus, often respond very well to physiotherapy, especially in those without significant functional weakness or rapid symptom progression. Larger tears, or those involving the infraspinatus or subscapularis, are more likely to be associated with functional deficits and may require surgical evaluation, particularly in younger or highly active individuals where biological healing and functional restoration are priorities.
Subscapularis tears deserve particular attention. As the anterior stabiliser of the shoulder, subscapularis damage can lead to internal rotation weakness, anterior shoulder instability, and a characteristic positive lift-off or belly press test on assessment. These tears, especially when large or involving the upper fibres, often carry a stronger case for surgical consultation.
Massive rotator cuff tears involving multiple tendons, particularly with associated muscle atrophy and fatty infiltration on MRI, present the most complex rehabilitation picture. In these cases, the decision between conservative physiotherapy and surgical repair requires careful shared decision-making, taking into account the individual’s age, activity demands, and the quality of the remaining tissue.
It is important to emphasise that imaging findings must always be interpreted in the context of the individual’s clinical presentation. Rotator cuff tears including full-thickness tears are common incidental findings on MRI in people with no shoulder pain whatsoever. A tear on imaging does not automatically indicate the need for surgery. The clinical picture, functional impact, and response to well-directed physiotherapy are the most meaningful determinants of outcome.
5. Treatment Options for Rotator Cuff Related Shoulder Pain
The overwhelming body of evidence supports physiotherapy as the first-line treatment for the majority of rotator cuff related shoulder pain presentations, including many full-thickness tears. Surgery is generally reserved for cases with significant functional deficit, failed conservative management, or acute traumatic tears in young, active individuals where early surgical repair may yield superior outcomes.
Graded-loading exercise stimulates tendon fibroblast activity, collagen synthesis, and tissue remodelling and is the biological foundation of tendon rehabilitation. Appropriately dosed, progressive loading of the rotator cuff tendons does not cause harm; it drives adaptation and recovery. The key is identifying the right exercises, at the right load and volume, at the right stage of rehabilitation.
At London Sports Physiotherapy, our comprehensive and individually tailored treatment approach may include:
- Manual therapy to restore glenohumeral and scapulothoracic mobility, address thoracic stiffness that commonly contributes to shoulder dysfunction, and reduce pain.
- Progressive rotator cuff and periscapular strengthening targeting the specific muscles identified as deficient on assessment, commonly the external rotators, lower and mid trapezius, and serratus anterior, to restore the force couple mechanism and normalise glenohumeral mechanics.
- Acupuncture and dry-needling to reduce muscle tension particularly in the upper trapezius and cervical spine musculature that commonly create secondary issues leading to increased pain and discomfort.
- Occlusion Blood Flow Restriction (BFR) Training is particularly valuable in the context of rotator cuff rehabilitation, where pain and disuse often lead to significant muscle atrophy. BFR allows meaningful gains in muscle strength and hypertrophy to be achieved at very low training loads, making it ideal for early and mid-stage shoulder rehabilitation where heavier resistance may not yet be appropriate or tolerated.
- Electrical Muscle Stimulation (EMS) to address rotator cuff and deltoid inhibition and facilitate neuromuscular re-activation, particularly in the early stages following injury, surgery, or prolonged disuse.
- Postural and movement retraining addressing scapular dyskinesis, thoracic kyphosis, and faulty movement strategies that place excessive demand on the rotator cuff during everyday activities and sport.
- Corticosteroid injections into the subacromial bursa to rapidly reduce inflammatory pain and facilitate earlier participation in rehabilitation — particularly useful in the acute or acutely flared phase, where pain is limiting the ability to engage meaningfully with exercise.
- Hyaluronic acid injections to improve the quality of the joint environment and reduce pain in those with co-existing glenohumeral joint degeneration, providing a longer-duration benefit compared to steroid for appropriate candidates.
6. Surgical intervention
We have excellent contact-links with top Orthopaedic shoulder consultants in the local area of Sutton and South London, both in the NHS and privately in hospitals such as Shirley Oaks and Spire St. Anthony’s. This is due to our many years of experience working in the NHS and private sector in the Sutton and South London areas. A surgical opinion is just a phone call away, and we ensure close liason with Orthopaedics both pre and post-surgically too.
At London Sports Physiotherapy we have aligned ourselves with leading Orthopaedic consultants in London. You will notice we are clinic partners with many top consultants including Mr Bobby Anand (Surrey Knee Surgeon), Mr Rhee (Shoulder and upper limb surgeon), Mr Mohan (Shoulder and upper limb surgeon), Mr Kunasingam (Foot and Ankle surgeon), Mr Kotrba (Spinal surgeon) and Dr Gautham Srinivisan (Pain consultant).
7. How Can London Sports Physiotherapy Help?
London Sports Physiotherapy is a specialist clinic with extensive expertise in the assessment and treatment of rotator cuff related shoulder pain. We understand that shoulder pain can be profoundly limiting, affecting sleep, work, sport, and the simplest daily tasks, and we are committed to delivering the highest quality clinical care to every individual who comes to us for help.
Our expert physiotherapists combine meticulous clinical assessment with the most advanced rehabilitation technology available. VALD dynamometry provides objective, data-driven strength measurement that guides and tracks your recovery with precision. BFR training and EMS allow us to rebuild rotator cuff strength and neuromuscular function at every stage of rehabilitation, even when conventional loading is not yet possible. Our injection therapy service delivers fast, targeted pain relief and optimises the biological environment for rehabilitation to take full effect.
We specialise in shoulder injuries and understand the critical distinctions between different presentation, from tendinopathy and bursitis through to partial and full-thickness tears at varying locations, that determine the most appropriate treatment pathway for each individual. Our approach is never one-size-fits-all; it is built entirely around your anatomy, your symptoms, your functional goals, and your life.
Whether you are an overhead athlete at a London sports club, a professional whose work demands repetitive arm use, or someone who simply wants to sleep through the night without shoulder pain, London Sports Physiotherapy has the expertise, technology, and clinical excellence to help you recover fully and durably.
Other common injuries of the shoulder complex include osteoarthritis, frozen shoulder, sub-acromial pain syndrome, bursitis, dislocation and fractures. For information on these injuries please click on the above links or return to the LSP Academy section.
Frequently Asked Questions
No. The majority of rotator cuff tears including many full-thickness tears respond very well to expert physiotherapy. Surgery is generally considered when there is significant functional weakness that does not improve with rehabilitation, an acute traumatic tear in a young active individual, or a massive multi-tendon tear with associated muscle atrophy. Your physiotherapist will help you understand which category applies to your presentation.
Full-thickness tears have limited intrinsic healing capacity due to reduced tendon vascularity. However, pain and function can improve substantially through physiotherapy even without anatomical healing of the tear. Surrounding muscles compensate, mechanics improve and the nervous system adapts. Partial tears have greater healing potential, particularly when blood supply to the area is supported through appropriately progressive loading.
Most shoulder pain does not need a scan straight away, as many conditions can be diagnosed with a clinical assessment. However, if your symptoms are persistent, unclear, or not improving, imaging can help confirm the diagnosis and guide treatment.
We offer convenient in-house point-of-care diagnostic ultrasound allowing for fast, accurate assessment without the need for external referrals so you can get answers and start the right treatment sooner.
Recovery depends on the severity and location of the pathology, chronicity of symptoms, and individual factors. Mild tendinopathy may resolve in 6–10 weeks. More significant partial or full-thickness tears typically require 3–6 months of structured rehabilitation. Your physiotherapist will provide a personalised timeline based on your assessment.
The supraspinatus is the most commonly torn tendon and primarily causes pain and weakness with shoulder elevation. Subscapularis tears affect internal rotation and anterior shoulder stability, and carry a higher likelihood of requiring surgical evaluation, particularly when the tear is large. Accurate clinical assessment and imaging are essential to distinguish between them.
Night pain is a very common and characteristic feature of rotator cuff related shoulder pain, particularly tendinopathy and bursitis, and does not in itself indicate a serious condition. It arises due to increased subacromial compression when lying on the affected shoulder and changes in tissue fluid dynamics at rest. It typically improves substantially with targeted rehabilitation.
Blood Flow Restriction training involves applying a cuff to the upper arm to partially restrict venous blood flow during low-load exercise. This creates a metabolic environment that stimulates significant muscle strength and hypertrophy gains at much lower resistance levels than conventional training. It is an evidence-based technique that is highly effective for building rotator cuff and deltoid strength during early rehabilitation when heavier loading is not yet appropriate.
London Sports Physiotherapy is based in Sutton, South London. Get in touch today to book your comprehensive shoulder assessment and begin your personalised recovery programme.
London Sports Physiotherapy — Specialist Injury Clinic in London. Expert assessment, diagnostic ultrasound, state-of-the-art rehabilitation technology, and outstanding clinical care.