Osteoarthritis is one of the most common conditions we treat at London Sports Physiotherapy. If you have been told you have osteoarthritis, or you are experiencing joint pain and suspect it may be the cause, this guide is designed to give you a clear, evidence-based understanding of the condition and crucially, what you can do about it. The good news is that with the right approach, most people with osteoarthritis can significantly reduce their pain, improve their function, and continue doing the activities they love.
1. What Is Osteoarthritis?
Osteoarthritis (OA) is a degenerative joint condition characterised by the gradual breakdown of cartilage, the smooth protective tissue that covers the ends of bones within a joint. As cartilage wears down over time, the bones can begin to rub against one another, causing pain, stiffness, swelling, and reduced mobility. In some cases, bony growths called osteophytes (bone spurs) may develop around the joint, and the surrounding tissues can become inflamed.
OA is the most common form of arthritis in the UK. According to Versus Arthritis, over 10 million people in the UK are affected, and it is one of the leading causes of pain and disability worldwide. While it can affect virtually any joint in the body, it most commonly occurs in the knees, hips, hands, and spine.
It is important to understand that osteoarthritis is a progressive condition meaning it will progress over time. However increased pain is not inevitable, and with the right management many people experience a significant reduction in symptoms even as changes within the joint continue. Pain levels do not always correlate directly with the degree of structural change visible on imaging. This is one of the most empowering messages in modern OA research: you can feel considerably better even if your X-ray does not change.
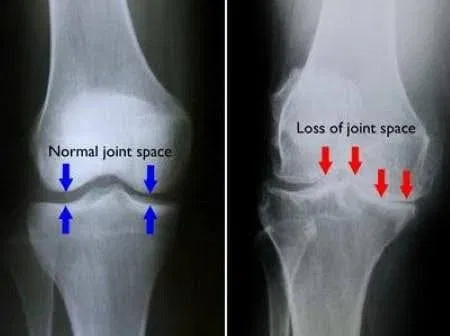
Below is an X-ray of a knee joint. On the left is a knee with well-preserved joint space and no evidence of osteoarthritis. On the right is a knee with significantly reduced joint space, indicating severe osteoarthritis.
2. What Causes Osteoarthritis?
Osteoarthritis does not have a single cause. It is a multifactorial condition influenced by a combination of biological, mechanical, and lifestyle factors. Understanding the risk factors can help put your diagnosis in context and inform the best approach to management.
The most commonly identified risk factors include:
- Age: The risk of OA increases with age as cartilage naturally becomes less resilient and the body’s ability to repair joint tissue diminishes. However, OA is not simply an inevitable consequence of getting older.
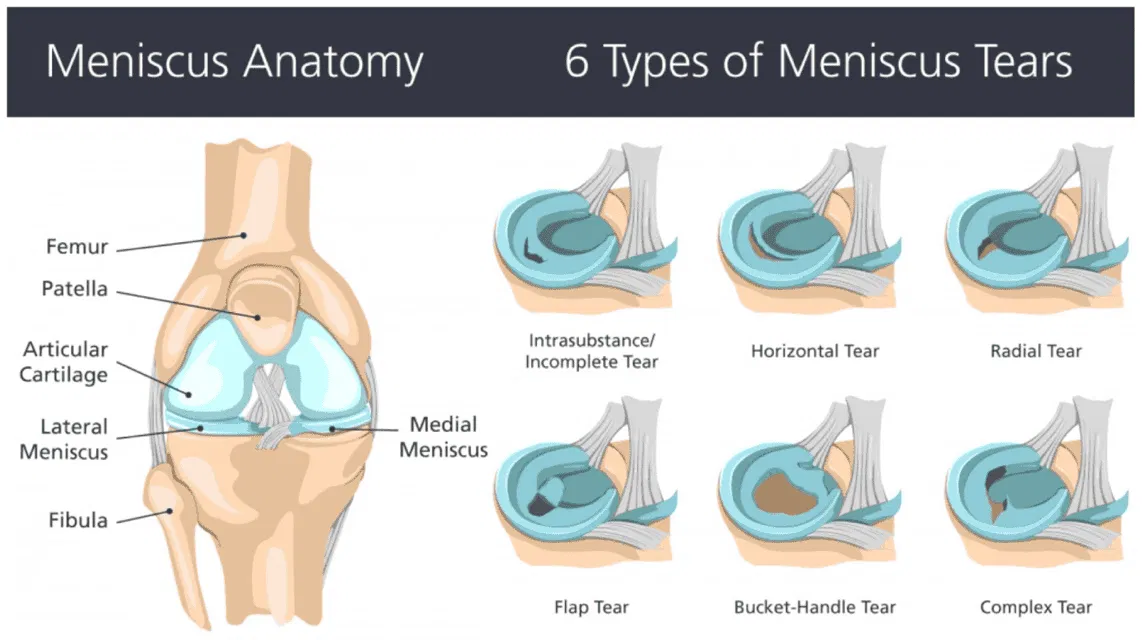
- Previous joint injury: A history of injury to a joint such as a ligament tear, meniscal damage, or fracture significantly increases the risk of OA developing in that joint later in life. This is particularly relevant in the sporting population.
- Body weight: Excess body weight increases the mechanical load on weight-bearing joints, particularly the knees and hips. Research suggests that being overweight can increase the risk of knee OA by up to four times.
- Gender: Women are more commonly affected by OA than men, particularly after the menopause, suggesting hormonal factors play a role.
- Genetics: There is a hereditary component to OA, particularly in hand and knee OA.
- Occupation and activity: Repetitive joint loading through certain occupations or sports can increase risk over time.
- Muscle weakness: Weakness of the muscles surrounding a joint, particularly the quadriceps in relation to the knee, is both a risk factor for and a consequence of OA.
Importantly, many of these risk factors, particularly muscle strength, body weight, and activity levels, are modifiable. This is where physiotherapy and structured exercise play a central and evidence-based role.
3. Signs and Symptoms of Osteoarthritis
The symptoms of osteoarthritis tend to develop gradually and vary considerably from person to person. Some individuals have significant structural changes on imaging with relatively mild symptoms, while others experience considerable pain and disability with more modest radiographic findings. This disconnect between imaging and symptoms is well-established in the research and reinforces the importance of treating the person, not the scan.
Common signs and symptoms include:
- Joint pain: Typically a deep, aching pain that worsens with activity and improves with rest, particularly in the earlier stages.
- Stiffness: Morning stiffness or stiffness after periods of inactivity lasting up to 30 minutes (in contrast to rheumatoid arthritis, where stiffness tends to last longer).
- Reduced range of movement: The joint may feel restricted, making everyday tasks such as climbing stairs, bending, or gripping more difficult.
- Swelling and warmth: Inflammation around the joint can cause visible swelling and a feeling of heat.
- Crepitus: A grating, creaking, or clicking sensation within the joint during movement.
- Muscle weakness: Particularly around the affected joint, which can further compromise joint stability and pain levels.
- Reduced function and activity: Pain and stiffness can limit participation in sport, exercise, and daily activities.
If you recognise several of these symptoms, particularly in a weight-bearing joint such as the knee or hip, it is worth seeking a professional assessment.
4. How Is Osteoarthritis Diagnosed?
Osteoarthritis is primarily a clinical diagnosis, meaning it is typically made on the basis of a thorough history and physical examination, without necessarily requiring imaging. NICE guidelines (updated 2022) recommend that a diagnosis of OA should be made clinically in adults aged 45 and over who have activity-related joint pain and either no morning stiffness, or morning stiffness lasting no longer than 30 minutes. In this presentation, imaging is not routinely required to confirm the diagnosis.
When a clinician assesses you for OA, they will typically evaluate your joint range of movement, muscle strength, functional ability, and pain behaviour. They may also assess your gait, posture, and the stability of the joint.
X-ray imaging is sometimes used to confirm the diagnosis or assess severity, and may show classic features such as joint space narrowing, osteophyte formation, and subchondral bone changes. MRI scanning is not routinely indicated for OA but may be used to exclude other pathology or assess the joint more comprehensively when the clinical picture is unclear.
It is worth emphasising again that imaging findings do not always predict your level of pain or functional limitation. Many people with severe OA changes on X-ray have manageable symptoms, and many people with mild radiographic changes experience significant pain. Treatment decisions should always be based on the whole clinical picture and not the scan alone.
5. Treatment Options for Osteoarthritis
The management of osteoarthritis has evolved considerably over the past decade, and the evidence now firmly supports a conservative, active approach as the first line of treatment. NICE guidelines are unambiguous on this point: exercise and physical activity are core, recommended treatments for all people with OA, regardless of age, pain severity, or radiographic changes.
Exercise and Physical Activity
Exercise is the single most effective intervention for osteoarthritis, supported by a large and consistent body of evidence. A common fear among people with OA is that exercise will accelerate joint damage or worsen their condition. The research is clear: this is not the case. Exercise does not damage arthritic joints. In fact movement is essential for joint health. Cartilage has no direct blood supply and relies on the compression and decompression of movement to receive nutrients and oxygen.
Multiple systematic reviews and meta-analyses have demonstrated that both aerobic exercise and resistance (strengthening) exercise significantly reduce pain and improve function in people with knee and hip OA. Strengthening the muscles around the joint particularly the quadriceps, hamstrings, and hip abductors for knee OA reduces the load transmitted through the joint and provides greater stability, leading to meaningful improvements in pain and quality of life.
Critically, pain can improve and often dramatically so, even as OA continues to progress structurally. This is one of the most important messages for people to understand. The goal of exercise-based management is not to reverse the structural changes within the joint, but to optimise the surrounding musculature, reduce load, improve movement quality, and recalibrate the pain system. The evidence consistently shows that this approach works.
Does Running Cause Osteoarthritis? What the Evidence Says
One of the most persistent myths about osteoarthritis is that running and high-impact exercise cause or accelerate joint damage. This concern is understandable, but the evidence does not support it. A landmark study by Hartwell et al. (2024), published in Sports Health, surveyed 3,804 marathon runners registered for the Chicago Marathon, the largest study of its kind ever conducted. The findings were striking: the cumulative number of years running, the number of marathons completed, average weekly mileage, and running pace were not significant predictors of hip or knee arthritis. The most significant risk factors identified were age, BMI, previous joint injury or surgery, and family history, not running history.
This study powerfully reinforces what the broader evidence base has long suggested: running does not inherently increase the risk of developing osteoarthritis. For the vast majority of people, staying active including running is safe, beneficial, and should be encouraged. If you have been told to stop running because of your joints, or if you are worried that exercise is making your OA worse, please speak to one of our physiotherapists. The evidence is firmly on the side of movement.
Weight Loss
Alongside exercise, weight management is one of the most powerful and evidence-based interventions available for osteoarthritis, and for overweight or obese individuals, it may be the single most impactful change they can make. The relationship between body weight and joint load is direct and measurable: research has established that every kilogram of body weight lost results in approximately a fourfold reduction in the compressive load through the knee joint with each step taken. Over the course of a day, the cumulative reduction in joint stress is enormous.
The evidence on how much weight loss is needed to produce meaningful clinical benefit is now well-established. The landmark IDEA (Intensive Diet and Exercise for Arthritis) randomised controlled trial by Messier and colleagues demonstrated a clear dose-response relationship between weight loss and OA outcomes. Participants who achieved at least 10% loss of their baseline body weight showed significantly greater reductions in pain, improvements in physical function, better health-related quality of life, reduced knee joint compressive forces, and lower levels of systemic inflammation, compared to those who lost less than 10%. A subsequent analysis confirmed that 10% weight loss represents a clinically important threshold, below this level improvements tend to be modest; at and above it, the benefits become substantial and meaningful.
Research also indicates that for every 1% of body weight lost, osteoarthritis pain, function, and stiffness scores improve by approximately 2%. This dose-response relationship means that even modest weight loss is beneficial but the greater the loss, the greater the reward. The combination of diet and exercise produces the most significant results, both in terms of weight loss achieved and in OA symptom improvement, compared to either approach alone.
NICE guidelines recommend that overweight and obese people with OA be supported to lose weight as part of their management plan. At London Sports Physiotherapy, we incorporate weight management advice and goal-setting into our treatment approach, and can refer to dietetic or medical support where appropriate. If you are carrying excess weight and have osteoarthritis, addressing this, alongside your exercise programme, can produce transformative results for your joint health and your quality of life.
Physiotherapy
Physiotherapy plays a central role in the NICE-recommended management pathway for OA. A qualified physiotherapist will design an individualised exercise programme targeting the specific impairments and functional limitations identified on assessment. This typically includes a combination of strengthening exercises, mobility work, neuromuscular training, and guidance on how to gradually increase activity levels safely and confidently.
Beyond exercise prescription, physiotherapy addresses pain education, helping people understand why their joint hurts, why movement is safe and beneficial, and how to self-manage their condition long term. Manual therapy techniques, such as joint mobilisation and soft tissue work, may also be used as adjuncts to reduce pain and improve range of movement, although the evidence is strongest for exercise as the primary intervention.
Acupuncture
Acupuncture can be a useful adjunct in the management of OA-related pain. A number of studies and meta-analyses have shown that acupuncture provides meaningful pain relief in knee OA, with effects that are both statistically significant and clinically relevant when compared to sham acupuncture and no treatment. The proposed mechanisms include the modulation of pain signalling pathways, reduction in local inflammation, and the release of endogenous opioids.
At London Sports Physiotherapy, acupuncture is used alongside exercise-based rehabilitation rather than as a standalone treatment. Used in this way, it can help to reduce pain sufficiently to allow people to engage more effectively with their exercise programme which remains the cornerstone of long-term management.
Steroid Injections and Hyaluronic Acid Injections
For those whose pain is not adequately controlled through exercise and physiotherapy alone, or for those who need a period of pain relief to engage effectively with rehabilitation, injectable treatments offer an additional option.
Corticosteroid (steroid) injections work by delivering a powerful anti-inflammatory agent directly into the joint. They can provide significant short-term pain relief often within days and are well-supported by evidence for knee and hip OA. NICE acknowledges their role in OA management, particularly where pain is the primary limiting factor. It is important to note that the effect is typically temporary (weeks to a few months), and they are best used as part of a broader management plan that includes exercise rehabilitation. Repeated frequent use is not recommended due to the potential for long-term joint tissue effects.
Hyaluronic acid (viscosupplementation) injections involve injecting a gel-like substance into the joint to supplement the natural synovial fluid, improving lubrication and cushioning. The evidence base is more mixed than for steroid injections, but several high-quality studies and meta-analyses support their use in knee OA, particularly for those who have not responded well to steroid injections or who are looking for a longer-duration effect. Some research suggests benefits lasting six months or more. They are generally well-tolerated and considered a safe option for appropriate people.
Both injection treatments work best when integrated into a comprehensive management plan. At London Sports Physiotherapy, we offer both steroid and hyaluronic acid injections with a view that injections as a bridge to rehabilitation, a tool to reduce pain sufficiently so that people can engage fully with the exercise-based treatment that will deliver lasting, long-term benefit.
6. How Can London Sports Physiotherapy Help?
At London Sports Physiotherapy we have extensive experience and specialist knowledge in the assessment and treatment of knee injuries and conditions, including osteoarthritis. We are specialists in managing knee pain and understand that living with OA can be frustrating, limiting, and at times disheartening, particularly for active individuals who simply want to get back to doing what they love. Our approach is evidence-based, patient-centred, and focused on giving you the tools and confidence to manage your condition effectively for the long term.
When you come to us with osteoarthritis, your treatment journey begins with a thorough clinical assessment to understand the extent of your condition, the joints affected, the impact on your function, and your individual goals. From this, we develop a personalised treatment plan that may include:
- A structured, progressive exercise programme targeting muscle strength, joint stability, and overall function, rounded in the latest evidence and NICE guidelines
- Hands-on physiotherapy including manual therapy and soft tissue techniques to reduce pain and improve movement
- Acupuncture to complement your rehabilitation and help manage pain
- Steroid or hyaluronic acid injections where clinically indicated, administered by experienced clinicians as part of a wider rehabilitation strategy
- Weight management guidance and support to help you achieve the clinically meaningful threshold of 10% body weight loss where appropriate
- Education and self-management guidance so you understand your condition, feel empowered in your recovery, and know how to maintain your progress independently
- Gait and movement analysis to identify and address any biomechanical factors contributing to joint load
We firmly believe, and the evidence strongly supports, that osteoarthritis does not have to mean the end of an active life. Pain can be reduced, function can be improved, and activity can be maintained and even increased, regardless of what your scan shows. The joint may change, but your quality of life does not have to.
If you are experiencing joint pain and would like a professional assessment, our experienced team at London Sports Physiotherapy is here to help. Contact us today to book your initial consultation and take the first step towards moving better and feeling better.
Frequently Asked Questions
Here we answer the questions we are most commonly asked about osteoarthritis at London Sports Physiotherapy.
This is one of the most common concerns we hear, and it is completely understandable. The reassuring answer, backed by a large body of research, is that exercise does not damage arthritic joints. Some discomfort during or after exercise is normal and expected, particularly when you are starting out or increasing your activity levels. A useful guide is the traffic light rule: mild to moderate pain during exercise (up to 4-5 out of 10) that settles within 24 hours is generally acceptable and does not indicate harm. If your pain is severe during exercise, or if it remains significantly elevated the following day, this is a signal to reduce the intensity or volume rather than stop altogether. The goal is to find a level of exercise that is challenging but manageable, and to build gradually from there. Your physiotherapist will help you find this balance and progress your programme safely.
The supplement market for osteoarthritis is vast, but the evidence is more limited than many manufacturers would suggest. Glucosamine and chondroitin are the most widely used supplements for OA, and while some studies have shown modest benefits for pain relief, particularly in knee OA, the overall evidence is mixed and NICE does not currently recommend them as a core treatment. Fish oil (omega-3 fatty acids) has some evidence for reducing joint inflammation and may provide mild symptomatic benefit. Vitamin D deficiency is common and has been associated with musculoskeletal pain; it is worth having your levels checked and supplementing if you are deficient. Turmeric (curcumin) has attracted interest for its anti-inflammatory properties, and some small studies show promise, though larger high-quality trials are still needed. In summary, no supplement has been shown to reverse or halt OA, and none should replace exercise and physiotherapy as the primary treatment. If you are considering supplements, speak to your GP or physiotherapist first, particularly if you are taking other medications.
Surgery is generally considered a last resort for osteoarthritis, recommended only when conservative treatments including physiotherapy, exercise, and injections have been thoroughly explored and have not provided adequate relief. The most established surgical option for severe OA is a total knee replacement (arthroplasty), most commonly performed on the knee or hip. Total knee replacement and total hip replacement are among the most frequently performed and well-studied surgical procedures in the world, with high success rates. The majority of people report significant reductions in pain and meaningful improvements in function and quality of life. Partial (uni-compartmental) knee replacement is an option for some where OA is confined to one part of the knee. Other procedures, such as arthroscopic surgery (keyhole surgery) to wash out the joint or trim torn cartilage, are not recommended for OA by NICE, as evidence shows they offer no significant benefit over non-surgical management. The decision to proceed with surgery should always be made jointly between you and your surgical team, with a clear understanding of the expected benefits, risks, and recovery process. Physiotherapy both before and after joint replacement is essential to optimise outcomes.
Currently, there is no cure for osteoarthritis in the sense that the structural changes within the joint cannot be fully reversed. However, this does not mean that your symptoms cannot be effectively managed or significantly improved. With the right combination of exercise, physiotherapy, lifestyle modification, and where appropriate, injections or other treatments, many people with OA experience substantial reductions in pain and improvements in function. The goal of treatment is not to cure the joint, but to give you the best possible quality of life and for the vast majority of people, that goal is very achievable.
Osteoarthritis is a progressive condition, meaning that changes within the joint can continue to develop over time. However, the rate of progression varies enormously between individuals, and many people experience long periods of stable symptoms. Importantly, structural progression does not always mean worsening pain. Research consistently shows that pain levels and X-ray findings do not reliably correlate. Regular exercise, maintaining a healthy body weight, and staying active are all factors that can slow progression and keep symptoms well-managed, even if the underlying joint continues to change.
You will often hear OA described as ‘wear and tear’, and while this gives a general sense of what happens in the joint, it is a somewhat misleading term. It implies that the joint is simply wearing out like a mechanical part, which can make people feel that the damage is inevitable and irreversible. In reality, OA is a dynamic process involving changes to cartilage, bone, synovial fluid, and the surrounding soft tissues. The joint has a degree of capacity to adapt and respond. Thinking of OA purely as wear and tear can discourage people from exercising, when in fact movement and loading, done appropriately, are exactly what the joint needs. We prefer to frame it as a condition that can be actively managed rather than one that simply happens to you.
Most people begin to notice meaningful improvements within six to twelve weeks of starting a structured physiotherapy and exercise programme, though this varies depending on the severity of the condition, how consistently the programme is followed, and individual factors such as age and overall health. It is important to have realistic expectations: the early stages of rehabilitation can sometimes feel challenging as the body adapts to new demands, and there may be some initial increase in muscle soreness. This is normal and does not mean the treatment is not working. Your physiotherapist will monitor your progress and adjust your programme over time to ensure you continue to move forward.
Short periods of rest during a flare-up of pain are reasonable, but prolonged rest is generally counterproductive for osteoarthritis. Joints need movement to stay healthy, and extended inactivity leads to muscle weakness, stiffness, and reduced joint nutrition, all of which can worsen symptoms over time. The modern evidence-based approach is to stay as active as possible, modifying the type or intensity of activity during a flare rather than stopping altogether. Low-impact activities such as swimming, cycling, or walking in water can be particularly helpful during periods of increased pain, as they allow you to maintain movement and fitness with reduced load through the joint.
Corticosteroid injections are generally safe when administered by an experienced clinician and used appropriately. They can provide significant short-term pain relief, often within a few days, and are well-suited to situations where pain is the primary barrier to engaging with rehabilitation. However, they are not recommended as a long-term or repeated strategy. Current guidance suggests limiting steroid injections to no more than three or four times per year in any single joint, as repeated injections at high frequency may have adverse effects on joint tissues over time. They are most effective when used as part of a broader management plan that includes exercise and physiotherapy.
Steroid (corticosteroid) injections work by delivering a powerful anti-inflammatory agent directly into the joint, reducing inflammation and pain relatively quickly. The effects are typically felt within days but are usually temporary, lasting weeks to a few months. Hyaluronic acid injections (viscosupplementation) work differently, they supplement the natural lubricating fluid within the joint, improving cushioning and reducing friction. The onset of benefit tends to be slower than with steroids, but the effects may last longer, with some studies reporting benefits of six months or more. The two injections are not mutually exclusive and may be recommended at different stages of your treatment depending on your response and clinical needs. Your clinician will advise which is most appropriate for you.
The majority of people with osteoarthritis do not go on to require joint replacement surgery. With appropriate conservative management such as exercise, physiotherapy, weight management, and where necessary, injections, most people can manage their symptoms effectively for many years without surgical intervention. Joint replacement is typically considered only when symptoms are severe, significantly impacting quality of life, and have not responded to a thorough trial of non-surgical treatment. If and when surgery does become a consideration, physiotherapy before the procedure can improve outcomes, and rehabilitation afterwards is essential for a successful recovery.
Yes, and in most cases, you should. Staying active is one of the most important things you can do for your joint health and overall wellbeing. The type and intensity of activity may need to be modified depending on the joint affected and the severity of your symptoms, but the goal should always be to keep you as active as possible. Many people with osteoarthritis continue to run, cycle, swim, play golf, and participate in a wide range of sports. Your physiotherapist can help you identify any biomechanical factors that may be contributing to your symptoms and work with you to find a way to continue the activities that matter most to you.
Yes, body weight has a significant impact on osteoarthritis, particularly in weight-bearing joints such as the knees and hips. Research shows that for every kilogram of excess body weight, the force transmitted through the knee joint during walking increases by approximately three to four kilograms. Even modest weight loss, as little as five to ten percent of body weight, has been shown to produce meaningful reductions in knee pain and improvements in function. Weight management is therefore an important component of OA management, and your physiotherapist or GP can help you find an approach that is realistic and sustainable for you.
There is a great deal you can do at home to complement your clinical treatment and keep your symptoms well-managed. Staying active and completing your prescribed exercise programme consistently is the single most important thing. Beyond this, maintaining a healthy body weight reduces load on the joints, and eating a balanced anti-inflammatory diet rich in vegetables, oily fish, and whole grains may offer modest additional benefits. Heat can be helpful for stiffness and muscle tension, while ice packs can help manage flare-ups of swelling and acute pain. Good sleep hygiene is important, as poor sleep can amplify pain. Assistive devices such as a walking stick, supportive footwear, or knee braces may help in certain situations, your physiotherapist can advise on what is appropriate for you.
The cost of a steroid injection is £180, while hyaluronic acid injections are £280. Please contact London Sports Physiotherapy directly to discuss which treatment option may be right for you. We will always ensure that any recommended treatment is clinically appropriate and represents the best value for your recovery.
London Sports Physiotherapy is based in Sutton, South London. Get in touch today to book your comprehensive knee assessment and begin your personalised recovery programme.
London Sports Physiotherapy — Specialist Knee Injury Clinic in London. Expert assessment, diagnostic ultrasound, state-of-the-art rehabilitation technology and outstanding clinical care.